

There are plenty of things in this world that I don’t pretend to understand. Things like “why does Glenn Beck unironically wear unlaced Chuck Taylors with a sport coat?” and “why, exactly, is Kim Kardashian famous” top the list, but I also realize that there are a number of non-trivial matters on which I am not an expert. When discussing one of these topics with someone who is, I will generally ask a lot of questions and attempt to get a handle on the material, and I will defer to many of his or her conclusions on the important points, at least until such time as I know enough to know better.
Some people choose to go a different route and argue about topics on which they have little to no grasp; David Meeks is part of this group. After my last reply, rather than have the intelligence to realize that he was incorrect on a number of his assumptions and that his proposed solutions might actually be faulty, Meeks fired back with what was, basically, a silly repeat of his previous posts/statements. He did not, however, post a link to this reply on Twitter or otherwise let me know that he’d written anything, which I found curious. Thankfully, a friend pointed me to the post.
With so little going on politically that doesn’t require me to write about Blanche Lincoln, I figured I’d return fire with a clusterbomb of my own.
Meeks writes:
Here is another post by a progressive blog:
http://www.bluehogreport.com/2010/06/24/state-hou-r-46-more-on-meeks-and-his-solutions/
And this post is yet another. I am the gift that keeps on giving.
I am posting this to help fellow conservatives see the arguments that the progressive side is making. We must be informed and be able to combat this way of destructive thinking.
Spoiler alert: I’ve read your entire post here and you “combat” these arguments like a band-aid combats a severed artery. You might want to pick a more attainable goal; perhaps you could say, “We must be informed and be able to see why our own arguments are ridiculous.” As for “destructive thinking,” I find it hilarious that logic, economic policy based on sound theory, constitutional arguments based on Supreme Court holdings, and general application of facts to your hyberbolic rhetoric strikes you as “destructive.”
Because I simply don’t have the time to write a big long post addressing every thing mentioned, I will just touch on a few below.
Counting the places where you quote me, this post runs 991 words. That is roughly three 8.5 x 11 pages typed in 12-point font, double-spaced, with one inch margins. Translation: You had the time to try to cherry-pick the points that I made that you thought you could rebut, and then you thought you would use your alleged lack of time as an excuse for why you didn’t address the other stuff, because the reality–that you had no response–made you look foolish.
Constitutionality of the Health Care Bill…
“I declare it as my opinion that [if] the power of Congress be established in the latitude contended for, it would subvert the very foundations . . . of the limited government established by the people of America.” James MadisonAs Thomas Jefferson affirmed, the federal government was “to certify with exact truth, for every vessel sailing from a foreign port, the state of health respecting this fever which prevails at the place from which she sails,” but that “the state authorities [are] charged with the care of the public health.” 13 Under the Constitution, states were to handle domestic health care issues, and the federal government foreign ones.
Please read more about the constitutionality of the healthcare bill and what our founding fathers said.
I thought you were going to address the constitutionality of the HCR bill. All you’ve done here is offer a couple quotes that have about as much bearing on whether the bill is constitutional as these:
“I have no voice in government, Waquine will get deported, and they’ll make him eat beets.” –ALF
“You say you want a revolution, well you know we all want to change the world.” –The Beatles
“Garth, marriage is punishment for shoplifting in some countries.” –Wayne Campbell
Less flippantly, I note that the Thomas Jefferson quote that you offered was taken out of context and does not make the point that you (or the website you took it from) attempts to make. (Please note, I actually use “out of context” correctly here, which is something you might try in the future. It’s a lot of fun.) Here is the original quote from Thomas Jefferson’s 1805 State of the Union address, in which he is discussing an unidentified epidemic that was then plaguing the United States.
Although from these facts it appears unnecessary, yet to satisfy the fears of foreign nations and cautions on their part not to be complained of in a danger whose limits are yet unknown to them I have strictly enjoined on the officers at the head of customs to certify with exact truth, for every vessel sailing for a foreign port the state of health respecting this fever which prevails at the place from which she sails. Under every motive from character and duty to certify the truth, I have no doubt they have faithfully executed this injunction. Much real injury has, however, been sustained from a propensity to identify with this endemic and to call by the same name fevers of very different kinds, which have been placed among those deemed contagious. As we advance in our knowledge of this disease, as facts develop the source from which individuals receive it, the State authorities charged with the care of the public health, and Congress with that of the general commerce, will become able to regulate with effect their respective functions in these departments. The burthen of quarantines is felt at home as well as abroad; their efficacy merits examination. Although the health laws of the States should be found to need no present revisal by Congress, yet commerce claims that their attention be ever awake to them.
Jefferson is saying (a) that, as more was known about the disease, the state authorities who dealt with public health (i.e., bodies like our modern DHS) and the U.S. Congress in its role as overseer of interstate commerce would be better able to do their jobs; and (b) that while Jefferson didn’t think there would be any need for Congress to review the states’ health laws, THE COMMERCE POWER REQUIRED THAT CONGRESS BE OPEN TO THE POSSIBILITY AND DO SO IF NECESSARY.
Part (b), in effect, takes your argument, lights it on fire, and dances naked around the rising flames in some sort of ritualistic pagan dance. As for part (a), what he most certainly is NOT saying is that the States alone are in charge of public health and that the Federal government may not intercede. Nor is he saying, as your statement attempts to, that Congress was responsible only for foreign health issues.
Additionally, the quote from Madison? Yeah, that had nothing to do with the commerce clause, under which I argued that the HCR bill was valid; Madison was referring to a broad expansion of the General Welfare Clause of the Tax and Spending Power in response to the Cod Fisheries Bill. A couple ironically funny points about you using this quote:
- In United States v. Butler, 297 U.S. 1 (1936), the Supreme Court rejected Madison’s exceedingly narrow definition of the general welfare clause, holding that the clause gives Congress the power to spend under the Tax and Spending power in areas that might not derive from other powers contained in the Constitution, so long as the spending was done in areas of national importance.
- Shortly after Butler, in Helvering v. Davis, 301 U.S. 619 (1937), the Court broadened the clause further, saying in essence that Congress may spend freely so long as it was done for the common good and was not specific to some local purpose.
So, not only is Madison’s quote not germane to our discussion, inasmuch as I said nothing about the General Welfare clause, but his position as defined in that quote has been directly rejected by the U.S. Supreme Court. Why does this matter? Because, to quote Marbury v. Madison,1 “It is emphatically the province and duty of the Judicial Department to say what the law is.” Which, again, is why I say that your citation to quotes is meaningless in this debate; the only relevant measurement for whether the law is constitutional is through application of Supreme Court case holdings.
As an aside, for someone who consistently whines about being taken out of context, even when you in fact were not, you sure seem willing to take the Founding Fathers out of context in your efforts to deify them. Weird. And what of Wall Builders, which Dave described to me on Twitter as (paraphrasing) “one of the most thorough and well-researched sites about our Founding Fathers?” Based on what Davey has put forth from Wall Builders here, I don’t think mangling the meaning behind obscure quotes from the men so as to “prove” your point and fulfill your agenda qualifies a site as a go-to source for information. So, new rule: quoting Wall Builders in a rebuttal to a point I’ve made automatically marks you as either a Republican shill or a moron (I’ll let you choose) and undermines the rest of any argument that you might make.
Deficithttp://blog.heritage.org/2010/06/10/the-more-we-learn-the-worse-it-gets/
Douglas Holtz-Eakin, of the American Action Forum, has released a new study that shows some 35 million Americans will get bumped from job-based coverage under the new law and be forced into the new government-managed system. That’s because the massive new subsidies promised by the government will make dropping insurance unavoidable for thousands of employers. He also predicts the migration out of employer plans will drive up the overall federal costs dramatically, adding another $500 billion over ten years to the costs projected by the Congressional Budget Office for the bill.
Perhaps that why CBO’s Director, Doug Elmendorf, is saying that the federal government’s health costs are still unsustainable, even after passage of the new law, despite repeated presidential promises that ObamaCare would solve our budget problems by painlessly “bending the cost curve.”
Another good post on the costs of the new healthcare law:
http://blog.heritage.org/2010/06/02/morning-bell-obamacares-true-costs-coming-to-light
The “findings” by Holtz-Eakin that your link cites is, to put it bluntly, a load of garbage, riddled with irrelevancies, half-truths, and outright lies. And you don’t have to take my word for it; two noted economists have said as much.
First, Paul Krugman:
OK, I finally got around to reading Douglas Holtz-Eakin’s op-ed on health care reform. It’s much worse than I thought; time to scratch Holtz-Eakin off my shrinking list of reasonable, reasonably honest conservatives.
How bad is it? Holtz-Eakin declares that
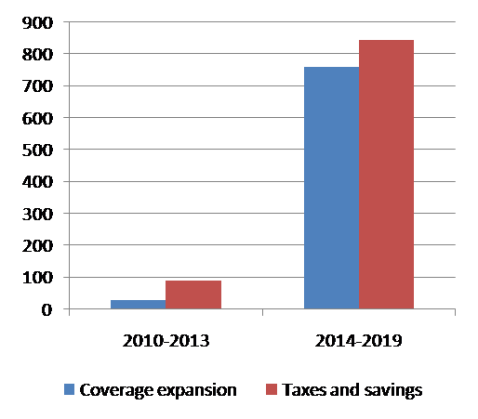
Gimmick No. 1 is the way the bill front-loads revenues and backloads spending. That is, the taxes and fees it calls for are set to begin immediately, but its new subsidies would be deferred so that the first 10 years of revenue would be used to pay for only 6 years of spending.
I think that’s what is technically known as a “lie”. Holtz-Eakin, of all people, knows how to read a CBO report. So he’s perfectly capable of looking at the actual report (pdf) and seeing that the revenues, like the costs, are minimal for the first four years. Here’s the chart:
CBO His implication that there’s funny business going on is totally false, and he knows it.
Wait, it gets worse: Holtz-Eakin implies that there are hidden, delayed costs:
Consider, too, the fate of the $70 billion in premiums expected to be raised in the first 10 years for the legislation’s new long-term health care insurance program. This money is counted as deficit reduction, but the benefits it is intended to finance are assumed not to materialize in the first 10 years, so they appear nowhere in the cost of the legislation.
Claims that the plan is window-dressed to look good in its first decade only to go sour later might sound plausible – except for the fact that the CBO projects bigger deficit-reduction in the second decade of the reform than in the first decade, something that wouldn’t happen if lots of costs were being hidden by being pushed off into the future.
That said, we do learn something important from Holtz-Eakin’s article. If this is the best critique a conservative budget wonk can come up with – if deliberately misrepresenting how the legislation works is the only way to make it seem irresponsible – then the bill must be pretty sound in fiscal terms.

And, if you don’t favor Krugman, Brad DeLong also weighed in.
So for your rebuttal, we have Holtz-Eakin’s disingenuous and misleading op-ed, which Heritage Foundation falls all over themselves to cite as “proof” that the bill is flawed. In response, we have a Nobel Prize winner and a professor/visiting scholar for the San Francisco Federal Reserve bank saying that Holtz-Eakin is wrong, which, by extension, means that Heritage is wrong.
Yeah…I think I’m going to go ahead and tally that one under “Not Successfully Rebutted By Dave.”
Tort Reform
“Prior to establishing liability restrictions in 2003, Texas was a haven for big medical tort litigation, triggering a dramatic increase in medical malpractice insurance rates. As a result, doctors left the state. Out of the 254 counties in Texas, 99 lost at least one specialist. Unfortunately, the majority of specialists left rural counties, leaving no additional specialists in the area. Access to care and quality plummeted. In 2003, Texas took action by passing comprehensive medical liability reform. The results were outstanding. Malpractice premiums fell by 27 percent on average and 125 counties added a high-risk specialist. Health systems began saving millions in medical liability costs and reinvested those savings in technologies (such as electronic medical records) designed to improve quality of care.”
It is interesting that you continue to quote from the Heritage Foundation for two reasons: (1) acting like they are even remotely unbiased is laughable, and (2) the parts you quote here are, like the previous section, composed of lies and half-truths, which makes one wonder about someone who continues to proffer Heritage’s statements as proof of anything other than Heritage’s bias. Taking their statements about the success of Texas’ med-mal limitations one by one:
Malpractice premiums fell by 27 percent on average
Americans For Insurance Reform released a study that showed, among other things:
- Nationwide medical malpractice premiums, inflation-adjusted, are nearly the lowest they have been in over 30 years.
- Medical malpractice premiums are less than one-half of one percent of the country’s overall health care costs; medical malpractice claims are a mere one-fifth of one percent of health care costs.
- The periodic premium spikes that doctors experience, including the spikes seen in Texas and other states from 2002 until 2005, are not related to claims but to the economic cycle of insurers and to drops in investment income.
- Many states that have resisted enacting severe restrictions on injured patients’ legal rights experienced rate changes (i.e., premium increases or decreases for doctors) similar to Texas, i.e., there is no correlation between “tort reform” and insurance rates for doctors.
125 counties added a high-risk specialist
Heritage’s method of counting doctors must differ from other people’s, because that’s not what the Texas Observer found by, you know, actually looking at data and not just basing conclusions on conjecture and speculation.
Health systems began saving millions in medical liability costs
The same report cited above found that medical malpractice claims, inflation-adjusted, are dropping significantly, down 45 percent since 2000, and, in over 30 years, premiums and claims have never been greater than 1% of our nation’s health care costs. This is probably why J. Robert Hunter, who is Director of Insurance of the Consumer Federation of America (CFA), former Commissioner of Insurance for the State of Texas, and former Federal Insurance Administrator under Presidents Carter and Ford said, “If Congress completely eliminated every single medical malpractice lawsuit … overall health care costs would hardly change, but the costs of medical error and hospital induced injury would remain and someone else would have to pay.”
Additionally, the Center for Justice & Democracy noted that it was the nation-wide decrease in insurance premiums–not any state’s tort-reform or lack thereof–that caused any appreciable savings in health costs.
On my quote and Blue Hogs response:
“ANY sort of government run health care is not the solution. This kind of thinking is bad for America.”Interesting. I mean, our veterans get government-run healthcare. Is that bad for America? You did say “ANY sort,” so I assume that you think veterans’ health insurance and VA hospitals and whatnot are a bad idea. That’s a very strange position for a former soldier to take, Dave. And what of older Americans and Medicare? Is that also a bad idea? I’ll be honest; I worry that you are letting your desire to sound forceful and enlightened get in the way of your ability to actually think about what you’re typing.
Progressives are good at taking things out of context. When this was written, the debate was what form, if any, the government run healthcare would look like. My point was whether it was the public option or health exchange or whatever else that if it was run by the government it was not the solution.
Context again, Dave? First, review my explanation about what being taken out of context actually means.
Second, you are right, in a grammatically challenged sort of way, that the discussion was what form the program “would look like.” In that context, you said that “ANY sort of government run healthcare is not the solution.” My question about the VA and Medicare was designed to test the limits of your absolute statement just as my question about the death penalty was designed to test the limits of your “life is life, I can’t in good faith make exceptions” statement. Implied in my question in both circumstances was “are you willing to take that statement to its logical conclusion, or are you selectively choosing only the activities that you disagree with?” Your incessant cries of “WAHHHH, CONTEXT!” suggest the latter.
Oh, and as long as we’re making blanket statements about what people are “good” at, I have one: conservatives are good at not being good at debating an issue without resorting to talking points and citations to biased, unfounded opinion as “proof.”
And yes I believe in the case of Medicare, it can be done better, more efficiently, and less costly if we transitioned it over to the free market.
I have a question for you. While it might seem rude, it’s a legitimate query. Are you being intentionally obtuse, or are you actually this bad at debate in a written form? Because those are the only two ways I think of that would make you think that your response here is meaningful without also addressing my broader point, which applied to many if not all of your proposed solutions, that there is no “free market” for healthcare.
Again:
This is probably better addressed in a separate post, so as to not get too far astray here, but here’s the Reader’s Digest condensed version: Most markets for health insurance in the U.S. are dominated by one or two companies, who collude to increase their income, decrease their payouts, and protect themselves from competition. This oligopoly colludes to keep prices high, choices low, payouts at a minimum, and new competitors from entering. The same goes for the pharmaceutical industry, where patents make some drugs available only from one company, where a few gigantic firms dominate almost all of the market, and where — thanks to President G.W. Bush — U.S. law forbids our government from securing lower prices (destroying the idea of economies of scale) for bulk government purchases for use by VA hospitals and the like. Access to hospitals is similarly limited so as to preclude any sort of real competition, which is essential for a free market.
In addition, I did not say that it couldn’t be done better or more efficiently; I asked whether you thought government-run healthcare in the form of Medicare was a bad idea. Look at it this way: imagine I ask someone who knows you, “Would it be a bad idea for the people of Dist. 46 to elect David Meeks?” A reply of “well, there are definitely better choices” doesn’t really answer the question because the question was not how you compared with an ideal candidate (or how Medicare compares with an ideal program), but whether it is a bad idea to choose you (or a bad idea to have Medicare).
HSA’s [sic]
Notice there he uses the old rich vs poor example. What he doesn’t realize is that middle class families can actually benefit from this quite a bit. I actually have an HSA that I put money into and people that know me know I am not rich.
Well throw me on a beach, and call me “Sandy!” If your single, anecdotal experience suggests that HSAs are good for the gander, then who am I to disagree?
Oh, wait, that’s right — I’m someone who tries his best to avoid logical fallacies.
I used the rich versus working poor distinction to illustrate that, for a number of people, the opportunity to have an HSA is worthless. Just because you, a person in his mid-30s who only recently got married, have the expendable income to contribute into your HSA does not mean that a lot of people — most notably the demographic who would qualify for the Medicaid expansion under the HCR bill — have the same situation.
The bigger point, however, that you choose to ignore (either because you lack an anecdote that supports your position or because you are starting to realize that your economic knowledge is minimal) is that HSAs are a bad idea as a widespread solution from an economic standpoint. As I stated before,
Also, get this, Dave: HSAs, because they disproportionately favor the wealthy by encouraging them to put pre-tax money in the account, would cost the federal government billions of dollars in lost tax revenues, thereby increasing the deficit (as the government will have to make up some or all of that money somehow). Yet you were against the HCR bill because you though — incorrectly, I might add — that it would add huge amounts to the U.S. deficit.
I guess you didn’t have time to get to those points. Good thing your schedule permitted you to regale us with another Life Story, by Dave.
MEDICAL VOUCHERS AND GROUPS
He missed the part that people could use these vouchers in conjunction with an HSA. Buy a high deductible plan and put the rest into an HSA which builds overtime [sic] or go out and purchase a plan that better suits your needs then [sic] the one the employer offers.
Someone now in a small business that has maybe 5 employees might join a church group that has 100 people and save money because they are in a bigger group. You could also join a Southern Baptist or Catholic Group that has millions. How about adding health insurance to your car insurance and getting a discount that way? The possibilities are endless.
Actually, I didn’t miss that part; the objections I raised to these “solutions” were not impacted by the possibility of using your first flawed solution in conjunction with them. Re: vouchers, I asked:
Those questions still stand. Even if I wanted to follow your example and buy a higher-deductible plan, the only way this idea works for all parties is if my higher deductible single-person (or single-family) plan, after accounting for dividend income from my HSA minus the difference in my deductible payments throughout the year, cost me less than my employer plan would have AND the vouchers cost my employer less than a company-based plan would have, because, without either of those factors, this plan leaves one or both of us worse off.
Beyond that, the fact that the “HSA builds overtime [sic]” is all well and good, but most families with young kids aren’t going to want to shell out $100 for a pediatrician visit rather than, say, $30 while they wait for their HSA to start showing results and saving them money in the longrun. Additionally, no one with a pre-existing condition that requires more-frequent doctor visits is going to be thrilled with paying significantly more in the immediate term, especially while the economy is bad and expendable income is at a minimum.
Back to my original objections: how will your plan not be worse for small businesses? I gather from your response that you think pooling of purchasers will somehow solve these issues. With respect to grouping of policies, I asked you:
Your response, such as it is, suggests that people could join a church group. Which, again, brings me back to the question of who would administrate a plan that “has millions” of potential members? Address the logistics of such a “solution,” and then I will tackle the rest of the problems with it.
(Aside: I noticed that you only used Christian churches in your example Dave. If I were trying to be like you — which, assuredly, I am not, as I loathe much of what you represent — here is where I would draw sweeping conclusions about “how conservatives think” or somesuch ridiculousness. But I digress.)
DOCTORS
Do you not see a gigantic problem with having the person who is treating you and making decisions as to what procedures you might need also be in charge of your insurance? Do the words “conflict of interest” mean anything to you?
Or what if you live in a small town and only have access to a general practitioner, but you need to be seen by a specialist? Would the GP’s insurance cross over? Would you have to re-apply for insurance from the specialist? Why would the specialist, especially if he were, say, an oncologist, insure you when it is likely that you have a very serious pre-existing condition?
Apparently progressives think doctors are bad people who wouldn’t do the right thing.
You are ridiculous. For one thing, I don’t profess to speak for all progressives, nor would I want to. Unlike the small-minded Republicans such as yourself, I place no value on groupthink. Perhaps if you attempted to think for yourself instead of basing everything you believe on what Fox News, Wallbuilders.com, and other such outlets told you to think, you might actually avoid making most of the mistakes you continue to make.
No, it’s not that I think “doctors are bad people who wouldn’t do the right thing.” I think doctors, like anyone else, expect to be compensated for the care they provide, and I wouldn’t expect them to stay in the doctor business long if they were constantly expected to lose money by providing expensive tests of arguably limited utility. I also think that it’s ironic that someone who professes to be pushing “free market” solutions would, in those solutions, suggest that doctors would not be expected to put profits above patients.
And therein lies the conflict of interests that I originally brought up. As one commenter said a while back, for an example of why this plan might not be the best idea, look at what happened when the banking industry was left to regulate itself. Are we to assume that doctors are benevolent altruists while bankers are greedy capitalists? If that’s the case, it doesn’t speak well of your beloved (and fictitious) free market.
You could also expand this to include a hospital and group of doctors who are affiliated with the hospital.
Fantastic. Now what of people who don’t live within reasonable distance of a top-notch facility and are, instead, treated at a small local hospital? If they need to be seen at UAMS, does the insurance transfer? Or, as I have already asked, why would a doctor who, by nature of his very profession, could assume that you were afflicted with a deadly disease want to insure you?
Your solution is not flawed because of the number of doctors in the pool, genius; it’s flawed because you ask the same people who are providing care to also be the third-party financier of the treatment, thus creating a conflict where, at times, a doctor will have to choose between ordering another MRI (for example) or giving the patient some aspirin and sending him home. Allowing financial considerations to influence this decision, as they must in your solution, creates a situation where care, diagnosis, and even patient-doctor communication is bound to suffer.
To answer the second part, this is ONE solution. This solution may NOT be viable in some places.
You are partially correct, but you need to replace “may” with “is” and “some” with “any.” Then you should append something like “I only suggested it because I really have no clue how much of this works.”
5 U.S. (1 Cranch) 137 (1803)↩